

Almost everyone experiences a painful oral sore at some point, but dismissing them all as simple, temporary annoyances is a clinical misstep.
The oral cavity serves as a highly sensitive window into your systemic health. While the majority of mucosal lesions are entirely benign, recognizing the visual and physical distinctions among the different types of mouth ulcers is critical for distinguishing a standard inflammatory response from a condition requiring biopsy.
If you are actively seeking expert Mouth Ulcers Treatment, the most important concept to grasp is this: an ulcer is rarely a standalone disease. It is a biological indicator.
The universal standard in oral pathology is the “two-week rule.” Any oral sore, whether it presents as a shallow white crater or a velvety red patch that does not completely resolve within 14 days, mandates a professional clinical evaluation.
We approach oral lesions through the lens of objective diagnostics rather than generic symptom management. By understanding exactly what these lesions look like and how they behave, you can eliminate the anxiety of the unknown and know exactly when it is time to step into the clinic. Whether you need routine evaluation or specialized mouth ulcer treatment in HSR Layout and Koramangala, early diagnosis is the key to protecting your oral and overall health.
Understanding Aphthous Ulcers

Among the various oral lesions, recurrent aphthous stomatitis, universally referred to as Canker Sores, represents the most frequent inflammatory complaint encountered in dental pathology. Statistically, up to 20% of the general population will experience these painful, non-contagious eruptions at regular intervals.
While they are highly disruptive to eating, speaking, and swallowing, aphthous ulcers are fundamentally benign. They are not viral, they cannot be transmitted through saliva, and they are entirely unrelated to the herpes simplex virus (cold sores), which typically form on the exterior of the lips.
To determine if your oral lesion is a standard aphthous ulcer, our diagnostic team looks for a highly specific visual anatomy.
The Visual Anatomy of a Canker Sore
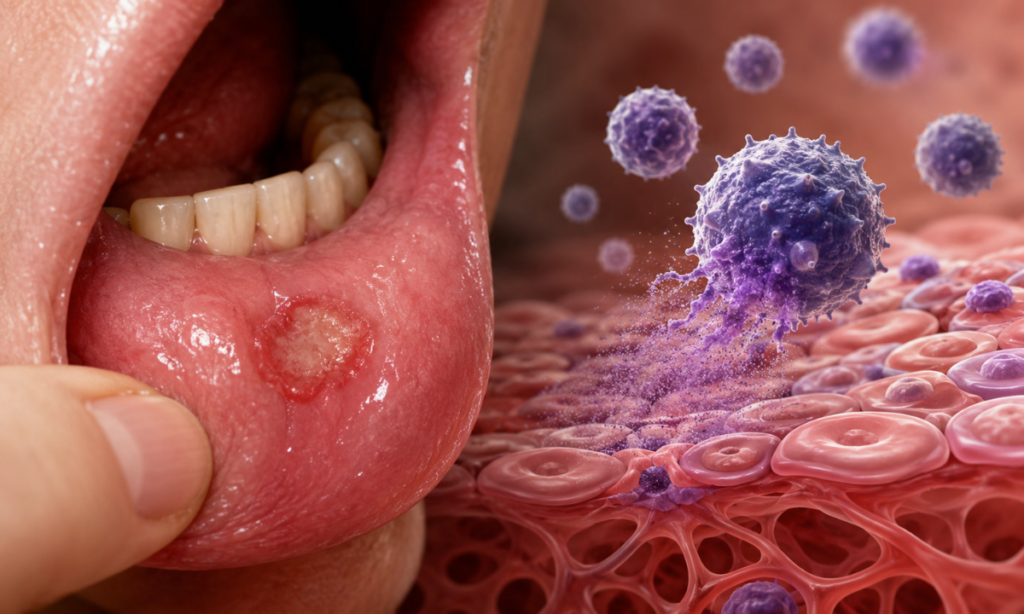
An active aphthous ulcer behaves like a localized inflammatory crater. If you examine the tissue closely in a mirror, a classic presentation will feature three distinct anatomical zones:
1. The Central Base: A shallow, depressed crater that appears pale white, yellowish, or grey. This color is actually a fibrinous slough, a temporary biological bandage made of dead white blood cells and proteins.
2. The Inflammatory Halo: A sharply defined, bright red perimeter surrounding the white center, indicating active blood flow and acute localized inflammation.
3. The Location: They strictly develop on the non-keratinized (soft and movable) mucosal tissues. You will find them on the inside of the cheeks, the inner lips, the soft palate, or the underside of the tongue. They rarely form on the hard palate or the firm gums directly wrapping the teeth.
Clinical Classification: Minor vs. Major Lesions
Not all aphthous ulcers behave the same way. Dentists classify these sores into three primary categories based on their size, depth, and healing trajectory:
| Ulcer Classification | Clinical Presentation | Healing Timeline & Scarring Risk |
| Minor Aphthous Ulcers | The most common variant (80% of cases). Typically oval-shaped, measuring less than 10mm in diameter. Pain is moderate but manageable. | Resolves spontaneously within 7 to 14 days. Leaves absolutely no structural scarring. |
| Major Aphthous Ulcers | Larger, deeper, and highly asymmetrical. Often exceeding 10mm in diameter. The pain is severe, frequently causing difficulty in swallowing. | It takes 2 to 6 weeks to fully heal. High probability of leaving permanent fibrous tissue scarring. |
| Herpetiform Ulcers | Rare. Presents as dozens of pinpoint, millimeter-sized lesions that merge into one large, jagged, and agonizing ulcer cluster. | Resolves in 10 to 14 days. (Despite the name, these are not caused by the herpes virus). |
Why Do They Form?

The exact autoimmune mechanism that causes the mucosal tissue to suddenly break down remains heavily debated in the medical community. However, clinical data points to a precise combination of environmental triggers and systemic vulnerabilities:
1. Mechanical Micro-Trauma: Accidentally biting the inner cheek, friction from a sharp broken tooth, or microscopic tears caused by stiff toothbrush bristles.
2. Chemical Irritants: Sustained exposure to Sodium Lauryl Sulfate (SLS), a common foaming agent found in commercial toothpastes, strips the protective mucosal barrier.
3. Nutritional Deficits: Chronic shortages of Vitamin B12, folic acid, zinc, or elemental iron directly compromise cellular regeneration in the mouth.
4. Systemic Stress: High cortisol levels induced by psychological stress severely depress the immune response, triggering an outbreak.
Clinical Intervention Guideline: If your ulcer fits the description of a ‘Minor’ lesion, standard palliative care, such as avoiding acidic foods and using an over-the-counter medication is sufficient.
However, if you develop a ‘Major’ ulcer that causes debilitating pain, visiting the clinic is highly recommended. We can prescribe targeted topical corticosteroids or utilize low-level laser therapy to instantly seal the nerve endings and accelerate tissue regeneration.
The Immunological and Autoimmune Manifestations
While aphthous ulcers are typically isolated reactions to temporary stress or trauma, other oral lesions signal a much deeper systemic misdirection. In these instances, the sore is not caused by an external irritant, but rather by the body’s own immune system mistakenly identifying the healthy mucosal cells of the mouth as a foreign threat.
When T-lymphocytes (specialized white blood cells) launch a localized attack on the oral lining, the resulting lesions require a completely different diagnostic and therapeutic approach. The most prevalent condition in this immunological category is Oral Lichen Planus.
Decoding Oral Lichen Planus (OLP)
Oral Lichen Planus is a chronic, non-contagious inflammatory condition. Unlike a canker sore that erupts and vanishes in a week, OLP is characterized by ongoing flare-ups and remissions. Because it mimics several other high-risk mucosal diseases, attempting to self-diagnose this condition is a dangerous gamble.
To a specialized oral pathologist, OLP presents in two distinct clinical forms, each requiring its own specific management protocol:
1. The Reticular Form
This is the most common and easily identifiable presentation of the condition.
1. Visual Presentation: It appears as a network of slightly raised, lacy, white thread-like lines on the inner cheeks, gums, or tongue. Dentists refer to these distinct, web-like patterns as Wickham’s striae.
2. Patient Symptoms: Surprisingly, the reticular form is often entirely painless. Many patients have no idea they even have it until a dentist spots it during a routine checkup. You may only notice a slight roughness when running your tongue against the inside of your cheek.
3. Clinical Action: Because it is asymptomatic, it generally does not require aggressive medication, but it absolutely requires clinical logging and continuous monitoring.
2. The Erosive Form
When the immune response intensifies, the reticular white lines break down into the erosive form of the disease.
1. Visual Presentation: The mucosal tissue becomes severely inflamed, appearing as angry, bright red patches. Within these red zones, painful, shallow ulcers develop. The gums may appear raw, swollen, and prone to spontaneous bleeding (a condition known as desquamative gingivitis).
2. Patient Symptoms: This form is highly symptomatic. Patients experience severe burning sensations, making it difficult to eat spicy, acidic foods. Routine oral hygiene, like brushing, can become exceptionally painful.
3. Clinical Action: The erosive form demands immediate professional intervention.
Why Clinical Management is Mandatory?
There is currently no absolute cure for autoimmune conditions like Oral Lichen Planus, but it can be highly successfully managed. Our approach at DDC Smiles to OLP focuses on rapid symptom relief and long-term surveillance.
During an acute erosive flare-up, we utilize targeted topical corticosteroids and specialized immunosuppressant oral rinses to suppress the localized T-cell attack and force the condition back into remission.
Furthermore, patients with the erosive form of OLP have a slightly statistically higher risk of developing cellular dysplasia (abnormal cell growth) in the affected areas. Therefore, establishing a baseline with a trusted diagnostic clinic is essential for tracking any subtle tissue changes over the years.
The Pre-Malignant Warning Signs With Red and White Patches
While aphthous ulcers cause acute pain and autoimmune conditions cause chronic discomfort, the most clinically dangerous oral lesions are often the ones that cause absolutely no pain at all.
When cellular DNA inside the mucosal lining becomes damaged, often due to cumulative exposure to carcinogens like tobacco, betel nut, heavy alcohol consumption, or chronic physical friction, the cells begin to mutate and replicate abnormally.
These architectural tissue changes, known as dysplasia, typically present as distinct colored patches on the oral tissues. Recognizing these pre-malignant warning signs is the cornerstone of early oral cancer detection.
Identifying Thickened Tissue
The first major category of high-risk mucosal change presents as a stark white, thickened plaque on the inside of the cheeks, the floor of the mouth, or the lateral borders (sides) of the tongue.
Clinically, this is diagnosed as Leukoplakia.
1. The Defining Clinical Trait: Unlike a fungal infection (such as oral thrush), which also presents as a white coating, this specific type of lesion cannot be wiped or scraped away with a piece of gauze. It is firmly embedded in the tissue architecture.
2. The Texture: Over time, the surface may transform from smooth and flat to a hardened, leathery, or distinctly corrugated (wrinkled) texture.
3. The Risk Factor: While the majority of these white patches are completely benign hyperkeratosis (the mouth’s version of a protective callus), a significant percentage conceal underlying precancerous cellular changes. Because they are almost always painless, patients routinely ignore them for months, missing a critical window for preventive treatment.
High-Risk Velvety Lesions
If a white patch warrants clinical suspicion, a red patch demands immediate, urgent pathology screening.
When abnormal cells fail to produce keratin (the white protective protein) and instead form a highly vascularized, thinned-out layer of tissue, it presents as a bright, velvety red macule or plaque. In oral pathology, this is classified as Erythroplakia.
1. The Defining Clinical Trait: These lesions appear as intensely red, flat, or slightly depressed patches. Because the tissue barrier is compromised and heavily supplied with fragile blood vessels, these patches often bleed spontaneously if brushed or rubbed.
2. The Risk Factor: This is considered the highest-risk pre-malignant lesion in the oral cavity. Statistically, biopsy results for these velvety red patches reveal severe cellular dysplasia or early-stage carcinoma in situ (localized cancer) in an overwhelming majority of cases.
Speckled Patches
In some high-risk cases, the tissue will exhibit a combination of both cellular errors, presenting as a red patch speckled with distinct white nodules (Erythroleukoplakia). These mixed lesions carry a dramatically elevated risk profile and are immediately prioritized for biopsy by our diagnostic team.
The Golden Rule of Oral Pathology is that pain is not an accurate indicator of danger. A massive, agonizing canker sore is generally harmless, while a completely painless, silent red or white patch could be life-threatening.
Never wait for an unexplained color change in your mouth to “start hurting” before booking a consultation.
When to Seek Immediate Care
To summarize the clinical guidelines, you should bypass home remedies and immediately schedule a diagnostic consultation if you experience any of the following “red flag” symptoms:
1. The 14-Day Rule: The ulcer or lesion has been present for more than two weeks without showing distinct signs of shrinking or healing.
2. Painless Discoloration: You discover a firm white plaque or a velvety red patch that causes absolutely no pain.
3. Structural Changes: The sore is accompanied by a noticeable hardening of the surrounding tissue, a lump in the cheek or neck, or suddenly swollen lymph nodes.
4. Functional Difficulty: The lesion alters your ability to chew, swallow, or speak normally without severe physical restriction.
Your oral mucosa is a highly accurate barometer for your overall health. Do not ignore the warning signs it provides. If you have noticed an unexplained change in your oral tissues, contact DDC Smiles today.
Why Accurate Diagnosis Matters?
When you are dealing with a persistent oral lesion, the primary goal should never be to simply numb the pain; the goal is to achieve absolute diagnostic certainty. Attempting to manage a complex immunological flare-up or a pre-malignant patch with mouthwashes is not just ineffective; it delays critical clinical intervention.
Because DDC Smiles operates as a comprehensive Dental Hospital in Koramangala and HSR Layout, we possess the specialized infrastructure and multidisciplinary expertise required to safely manage complex oral pathology. Patients trust our facility for lesion diagnostics because we eliminate the guesswork:
1. Specialist-Led Evaluations: Your screening is conducted by highly trained specialists under the clinical direction of Dr H.J. Jaikrishna, ensuring that subtle mucosal changes are identified accurately.
2. Advanced Biopsy & Laser Capabilities: If a lesion requires a biopsy or immediate excision, we perform these procedures in-house using advanced soft-tissue dental lasers, which minimize bleeding, reduce structural trauma, and significantly accelerate your healing time.
In the presence of open oral wounds or immunological conditions, secondary infections are a major risk. Our rigorous sterilization protocol and Class B Autoclaves guarantee a hospital-grade, virus-free environment for every diagnostic procedure.
Conclusion
Your mouth is one of the most sensitive indicators of your overall well-being. While the vast majority of oral sores are completely harmless and will resolve on their own, a persistent, unchanging, or painless ulcer should never be ignored.
If you have noticed a lesion lasting longer than 14 days, do not wait for it to cause discomfort before taking action. Schedule a quick, stress-free diagnostic screening at DDC Smiles. Catching subtle tissue changes early, our specialists ensure your smile remains safe, healthy, and confident for years to come.
Reference:
1. https://www.betterhealth.vic.gov.au/health/conditionsandtreatments/mouth-ulcers
2. https://my.clevelandclinic.org/health/diseases/21766-mouth-ulcer
